
Friday Report: Issue 66  www.covid-arg.com
www.covid-arg.com
By: John Roberts, Adele Groyer and Matt Fletcher



COVID-19 Actuaries Response Group – Learn. Share. Educate. Influence.
COVID-19 is still one of the hottest topics for scientific papers and articles. The COVID-19 Actuaries Response Group provides a bi-weekly Friday update with a summary of key papers, articles and data.
Vaccines
Vaccine Progress
The latest progress on the “Spring Booster” campaign, as recorded in the weekly Flu & COVID Surveillance Report (link) is that over 50% of the eligible age cohorts (i.e. over 75) have now had the additional jab. This totals 2.7m, which suggests a rate of just under half a million jabs each week since the programme started in mid-March.
However, at the other end of the age range, the programme to give a first jab to the 5 to 11 age group continues to make very slow progress, with just 6% of the eligible population of 5m having been jabbed. The slow progress would appear to be a combination of ineligibility due to a recent infection, availability, and uncertainty amongst parents regarding the benefits of vaccinating their children.
Variants
Frequency of Sequences of Omicron Sub-lineages BA.2.12.1, BA.4 & BA.5
In Friday Report 65 (link) we gave an update on what was known about Omicron sub-lineage BA.2.12.1 which was being reported predominantly in the United States, as well as BA.4 and BA.5 which were reported largely in South Africa.
Nextstrain are now tracking these “clades” and CoVariants provides visualisations of the NextStrain data. Their charts show the proportion of total sequences that fall into the defined variant groups. It’s important to be aware that that sequenced samples may not be representative of total cases, and that the data is dependent on countries submitting samples to GISAID.
In the week 18 to 25 April, the following proportions of cases were noted:
| Variant Pango Lineage | NextStrain clade | Proportions of sequenced samples |
| BA.4 | 22A | South Africa: 38%
Botswana: 38% Austria: 3% |
| BA.5 | 22B | South Africa: 18% |
| BA.2.12.1 | 22C | USA: 17%
Austria: 5% Hong Kong: 1% Mexico: 1% |
Countries not specifically mentioned did not submit any cases from these sub-lineages in that week. To date, the UK has reported only a few confirmed or probable cases of these variants. (link)
CoVariants also provides visualisations by country and we reproduce a selection of their graphs showing the emerging BA.2.12.1 lineage in the USA (dark blue, top right of graph), and the emerging BA.4 and BA.5 lineages in South Africa (dark purple is BA.4 and blue is BA.5). The UK chart shows that sequences here are still dominated by BA.2 (light purple).



Properties of BA.4 and BA.5
A study from South Africa (link) explains that the spike proteins of BA.4 and BA.5 are identical, and comparable to BA.2 except for the addition of 69-70del, L452R, F486V and the wild type amino acid at Q493. The L452R mutation in particular may result in increased infectivity as it has been associated with an increased affinity for receptor binding. This mutation is present in Delta, Kappa and Epsilon variants and similar mutations have also arisen independently in at least four BA.2 sub lineages, including BA.2.12.1.
The study estimates growth advantages for BA.4 and BA.5 of 0.08 (95% CI: 0.07 – 0.09) and 0.12 (95% CI: 0.09 – 0.15) per day respectively over BA.2 in South Africa.
The paper explains that, while BA.4 and BA.5 are similar to BA.2, they are not thought to be descended from BA.2. Instead, Bayesian phylogenetic methods suggest that BA.4 originated around mid-December 2021 and BA.5 in early January 2022 with a common Omicron ancestor dating back to mid-November 2021.
Immune Escape of Omicron sub-lineages
A study from South Africa (link) examined immune escape properties of BA.4 and BA.5. This was done by comparing the neutralising ability of blood samples from participants against BA.1 and then against BA.4 and BA.5. There were 24 unvaccinated participants infected with BA.1 and 15 vaccinated participants who had a breakthrough BA.1 infection.
Importantly, absolute BA.4 and BA.5 neutralisation levels were about 5-fold higher among vaccinated than in unvaccinated participants, suggesting that vaccination conferred superior neutralisation ability than prior infection alone.
The same samples were also used to investigate neutralisation ability to various strains of COVID-19 and are reported in a separate article (link). Against all strains, samples from participants with hybrid immunity showed greater neutralisation than those from participants only with infection-induced immunity.

Sensitivity of Omicron Sub-Variants to Therapeutic Monoclonal Antibodies (link)
This study from Japan reports on the sensitivity of Omicron sub-variants to eight different monoclonal antibody treatments. Tests to determine the concentration at which 50% neutralisation of the virus could be achieved were conducted using pseudoviruses harbouring the spike proteins of these sub-variants. The key findings were:
- 2 and the new variants are resistant to most of the 8 monoclonal antibodies studied.
- Perhaps surprisingly, Bentelovimab is more effective against BA.2 and the Omicron subvariants than against the parental virus.
- Cilgavimab had similar effectiveness against parental, BA.2 and BA.2.12.1 viruses but is less effective against BA.4 and BA.5.
- Sotrovimab is less effective against BA.2 and its sub-lineages than against parental virus but has more neutralising ability against the new Omicron sub-lineages than against BA.2.

Another pre-print study from China (link) also suggests that Bentelovimab and Cilgavimab can still effectively neutralise BA.2.12.1, BA.4 and BA.5.
Medical
Solidarity Trial Shows Limited Benefit of Remdesivir (link)
A study across 35 countries randomly allocated over 8,000 hospitalised patients to receive remdesivir or a control between March 2020 and Jan 2021. The final results have now been published and the authors suggest that there was no mortality benefit in using the drug for those already receiving ventilation, and a small benefit for those receiving less invasive treatment.
A summary of the results is as follows, with the mortality ratio showing the mortality experience of the remdesivir-treated patients compared with that of non-remdesivir patients:
| Patient Category | Mortality ratio | 95% Confidence Interval |
| No oxygen | 0.76 | 0.46 – 1.28 |
| Oxygen, but not ventilated | 0.87 | 0.76 – 0.99 |
| Ventilated | 1.13 | 0.89 – 1.42 |
| All | 0.91 | 0.82 – 1.02 |

Note that the enrolment period for this study ended in January 2021, and thus its relevance to more recent strains of the virus is not known.
Data
US Study Shows Higher Vaccination Take-Up Reduces COVID-19 Mortality (link)
An analysis of US data in over 2,500 counties across 48 states has concluded that higher vaccination take-up resulted in reduced COVID-19 mortality during the Alpha and Delta variant periods, with a 10% improvement in take-up resulting in a 9% reduction in deaths. There was a similar reduction in cases, with a 7% reduction from a 10% increase in take-up.
Whilst the authors note that they allowed for variations such as social vulnerability (which includes many aspects of socio-economic status such as employment, disability and deprivation), they also note that differences in NPIs adopted (e.g. masking) were not considered.

ONS Infection Study (link)
The latest infection prevalence estimates from the ONS show continued rapid falls across the UK. Since our latest update the estimate for England has halved, with reductions of around one third in the three devolved administrations.
Reassuringly, these reductions are across all age groups, including the older age groups more vulnerable to serious illness.

ONS Antibody Study (link)
We have noted in previous Reports that the ONS had suggested that the threshold of 179ng/ml used in its antibody studies may be insufficient to provide an equivalent level of protection against Omicron as it did against previous variants. The latest update to the Antibody Study addresses this point, with the introduction of a new level of 800ng/ml. Determination of this level was, however, based on practical considerations regarding the ability to produce a retrospective time series, as opposed to any research on the level required.
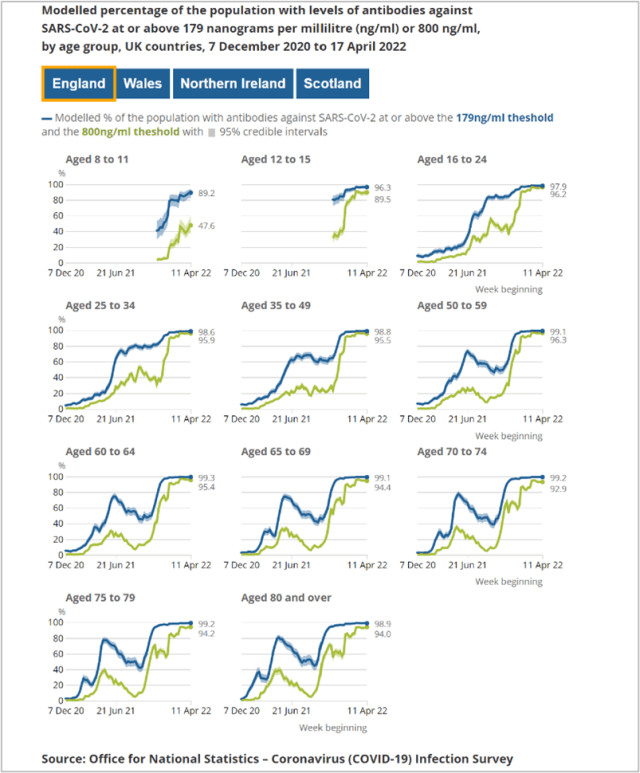
Even at this higher threshold, very high percentage levels are recorded at all but the youngest age groups, with an overall figure of around 95%, compared with 99% at the lower threshold.
With the Spring booster programme restricted to over 75s, it is possible to look for evidence in any divergence in antibody levels either side of 75. With that programme starting in mid March, there is some slight evidence that antibody levels have increased above 75 (as shown by the falling line below), but have fallen slightly below aged 75.

ONS Self-Reported Long Covid Study (link)
The ONS estimates prevalence of Long COVID by asking participants who previously tested positive in the ONS Coronavirus infection survey the question “Would you describe yourself as having ‘long COVID’, that is, you are still experiencing symptoms more than 4 weeks after you first had COVID-19, that are not explained by something else?”
The data is split by vaccination status at the time of testing positive, as well as by variant. Prevalence of both characteristics changes over time which makes interpretation complex. The results are adjusted for socio-demographic characteristics.

WHO Estimate of Global Excess Deaths (link)
A new estimate from the World Health Organisation suggests that excess deaths for 2020 and 2021 were in the order of 14.9m (range 13.3m to 16.6m), being 13% more than expected over the two years.
The BBC summary of the report highlights variations both in the level of excess (ranging from 437 per 100,000 in Peru to -28 in Australia), and in the comparison of the excess and reported COVID deaths. Using the latter metric, Egypt has an excess death rate which is more than 11 times their official COVID death rate.
Any analysis of excess deaths is inevitably just an estimate, and the need to use a consistent methodology across many countries is likely to increase the extent to which the result for any one country may be flawed. Indeed, the estimate for Germany appears to be significantly overstated, as the assumed baseline mortality for the two years appears too low.
Nevertheless, in aggregate it is a sobering statistic that over the last 22 months the pandemic may have led to (of the order of) 15m more people dying than would otherwise have been expected. (We plan to publish a more detailed bulletin on this report shortly.)
And Finally …
Brazilian Centenarian in Ninth Decade at Same Employer (link)
Several of the group focus on longevity in our day-to-day work, so we’re always interested in longevity related stories. We were interested to hear about Walter Orthmann, who has been working for the same company for over 84 years, and is now a Guinness World Record holder for length of time with one employer.
To think of this feat in another way, anyone starting work this month will need to remain with their employer until 2106 to break Walter’s record. Congratulations Walter on both your centenary and long service, and we hope you’ve had some long service awards along the way.

6 May 2022