
Friday Report: Issue 61
By: John Roberts, Adele Groyer and Matt Fletcher



COVID-19 Actuaries Response Group – Learn. Share. Educate. Influence.
COVID-19 is still one of the hottest topics for scientific papers and articles. The COVID-19 Actuaries Response Group provides a bi-weekly Friday update with a summary of key papers and articles.
Vaccines
Wales and Scotland Move First on Vaccination for Younger Children (link)
Speculation that there was to be an announcement last Friday from JCVI on its recommendation for 5 to 11 year olds was followed by news that the government was still considering its response. However, this week saw Wales then Scotland announce that it would follow the recommendation (which at that stage was yet to be published), and offer vaccines (two small injections of Pfizer) to this age group. This was then quickly followed by publication of the JCVI advice, with the UK government announcing that a “non-urgent” roll-out would begin in April in England.
The advice comments that it estimates that around 85% of children in the age group have already had a COVID infection, with around half of these occurring since Omicron took hold, i.e. in the last two months.
Italian Study of Myocarditis/Pericarditis following Vaccination (link)
A study of just under 3m people who received at least one dose of either of the mRNA vaccines confirms a heightened risk for those under 40 of myocarditis and pericarditis (as measured by requiring hospitalisation) shortly after administration of the vaccine. The study notes there was no heightened risk above age 40.
Notably the excess risk appeared lower for the Pfizer vaccine (Comirnaty) than for the Moderna vaccine (Spikevax) as shown in the table below, with no evidence of a heightened risk after the first Pfizer dose.
A pattern of increased risk in the younger age groups was seen, and for Moderna the excess risk was limited to males. (It should be noted though that the sample size for Moderna was around a fifth that for Pfizer, which may have limited the ability to detect statistically significant results.)
Only one death was observed out of 441 cases – this occurred 38 days after a pericarditis diagnosis which itself was 53 days after a second dose. The cause of the death is unknown, but the diagnosis was well outside the 0 to 7 days risk period post vaccination being analysed.
Finally, the study conclusion highlights the need to consider any increased risk in the context of the overall beneficial effect of the vaccine in preventing serious COVID-19 disease and death (for instance, see the study we summarise on page 3).
Variants
BA.2 Growth (link)
The latest Variant Technical Briefing continues to show that BA.2 has a transmission advantage over the original Omicron strain of BA.1. In the chart below (from link), BA.2 has grown to around 19% of those sampled by Feb 7th. (Note that more recent estimates (link) on Twitter put the figure as high as around a third.)
The briefing notes that the mean serial interval for BA.2 appears to be around half a day shorter than for BA.1 (3.3 days compared with 3.8), and this is likely to be the reason for the transmission advantage. However, there is no evidence yet that BA.2 is materially different in terms of vaccine escape or severity of outcomes, although simply by virtue of being more transmissible, it is likely to lead to a greater number of instances of serious illness than if BA.1 remains prevalent.

Clinical and medical news
Increased Risk of Heart Disease and Stroke post COVID Infection (link)
A study in Nature of over 150,000 US veterans reports a significantly increased risk of cardiovascular disease (including heart attack and stroke) in the first 12 months following infection with COVID, when compared with a control group of over 5m people.
Infections covered the period up to mid-January 2021, so will have been prior to the vaccination roll-out. In addition, cohort participants were censored at the point of a first vaccination dose, to avoid any risk that the vaccination itself triggered any heart-related illness. Finally, the first 30 days post infection were excluded to avoid any residual immediate effect from the period of infection.
The study reports an increased risk for all degrees of infection, with, as might be expected, a further heightened risk for those admitted to hospital in respect of their COVID infection, and another increase for those admitted to ICU.
Heightened risk was reported for all demographic factors (age, sex, race etc), regardless of whether these factors were ones typically associated with increased cardiovascular disease, with the aggregate increases as shown in the table below.

Paxlovid (Nirmatrelvir) Results Published (link)
We reported in issues 58 (link) and 59 (link) MHRA’s approval of Paxlovid, together with the government’s purchase of 2.75m courses. The trial results have now been published and confirm that when taken in conjunction with ritonavir, non-hospitalised higher risk patients had an 89% lower risk of progression to serious disease (defined as hospitalisation or death within 28 days).

RECOVERY Trial Reports on casirivimab and imdevimab Combination (link)
A study of the monoclonal antibody combination of casirivimab and imdevimab has shown that it has a beneficial effect on patients in hospital who have not mounted an antibody response on their own “seronegative”, but there was no equivalent benefit for those who are seropositive.

Nearly 10,000 patients were enrolled between September 2020 and May 2021, of which half received the treatment under investigation and half received usual care. Of those who were seronegative, the study showed an improvement in the 28 day mortality outcome of just over 20% (RR 0.79, CI 0.69 – 0.91), with the equivalent figures for seropositive patients being RR 1.09 (CI 0.94 – 1.25).
The study therefore recommends that patients undergo serological testing and that the treatment is limited to those shown to be seronegative. It notes that this has already been implemented in the UK based on the results of the trial.
Genetic Differences Influence Severity of Infection (link)
A study of over 2,000 critically ill patients over the period March to July 2020 has identified that a common variation of the TMPR552 protein (which is found in the lung, colon, stomach and many other tissues) results in a reduced risk of serious infection. This finding was then confirmed in other large COVID datasets.
The variant, rs12329760, which is found in around a quarter of the population, also appeared in tests to reduce the ability of TMPR552 to activate the viral spike protein, providing an explanation as to why individuals with the variant were less predisposed to serious infection.
However, it is noted that this effect appears to differ by variant. Whereas Delta is highly dependent on TMPR552 for cell entry, Omicron is not, and thus presence of the variant is unlikely to give the same protective effect as observed in the study (this may be a reason why Omicron appears to result in less severe illness than Delta).
The authors also observe that antivirals targeting the host protein might thus only work for infections with the variants that rely on TMPRSS2.
Implications of an Omicron Infection on Immunity to Other Variants (link)
We know from various studies that Omicron is much more able to escape existing immunity than have previous variants. A study in South Africa has investigated what immunity Omicron might offer against other variants.
Plasma from 27 individuals, 20 of whom were unvaccinated, was used to test in the laboratory the antibody response to Variants of Concern, including Omicron itself, Beta and Delta. Unsurprisingly, a good response was seen against a further infection with Omicron, but the response against other variants depended on vaccination status.
The conclusion drawn is that whilst an Omicron infection may provide additional natural immunity for those already vaccinated, it does not appear to confer an adequate degree of protection for those unvaccinated in respect of other variants. This should be an important consideration for any vaccine hesitant people who may believe that having been infected recently with Omicron that they are now protected against any future variants.
It should be noted that these lab tests only investigate one aspect of the body’s immune response, and it is possible that other immune responses offer greater protection.
COVID treatments available in the UK
Prospects for COVID patients continue to improve with a growing arsenal of treatments. A BBC article contrasts the situation in April 2020 when doctors had nothing but oxygen to treat critically ill patients to the range of drugs that are now available. According to the NHS the treatments available to people at risk of becoming seriously ill from COVID-19 are:
- Sotrovimab (Xevudy) – a monoclonal antibody which sticks to coronavirus to prevent an infection from getting established
- Nirmatrelvir and ritonavir (Paxlovid) – an antiviral
- Remdisivir (Veklury) – an antiviral
- Molnupiravir (Lagevrio) – an antiviral
A doctor or specialist needs to confirm who is eligible for treatment.
Additionally Dexamethasone – a cheap anti-inflammatory steroid – has proved to be effective at reducing mortality among hospitalised patients.
As reported in Friday Report 57, the ongoing PANORAMIC trial is investigating Molnupiravir. The trial is open to anyone that meets the following criteria:
- Currently experiencing COVID-19 symptoms, beginning in the last 5 days; and
- Have had a positive PCR or Lateral Flow test for COVID-19; and
- Aged 50 or over, or aged 18 or over with a listed pre-existing condition.
One of our team is now among the participants of this trial, having recently tested positive.
This is just one of a number of ongoing clinical trials in the UK. The DHSC-led COVID-19 Therapeutics and Antivirals Taskforce co-ordinates the UK’s research effort and, along with PANORAMIC, lists AGILE, RECOVERY, RECOVERY+, PRINCIPLE, PROTECT-V, HEAL and STIMULATE-ICP trials on its website. These trials consider COVID-19 treatments in the community, among hospitalised patients and among patients discharged from hospital. The trials also cover prophylactic treatments among immunocompromised patients as well treatments for those suffering from long COVID.
Modelling
We are now clearly past the peak of Omicron infection and hospitalisation so we will not publish our comparison of actual and modelled hospitalisation rates in this report. The peak daily number of hospitalisations was around half the figure set out in the modelled scenario (alternatively stated, another doubling of infections could have led to a peak close to the modelled outcome).
Data
ONS Infection Study (link)
The latest ONS infection prevalence data shows a small fall, after three weeks when downward progress was stalled if not reversed. There remains considerable difference in the four nations with Scotland increasing, Wales falling, and Northern Ireland out on a limb and much higher at 8%. Evidence that BA.2 has grown much more rapidly in Northern Ireland may be behind the disconnect with the rest of the UK, as shown in the second chart below.
After several weeks at exceptionally high rates, the prevalence in younger children has now started to fall, with the Age 2 to School Year 6 band falling over the last fortnight from 13% to 7.5%.
Given the comment earlier regarding vaccination for 5 to 11 year olds that over 40% have been infected since Omicron emerged, it is possibly unsurprising that prevalence is now falling quickly.

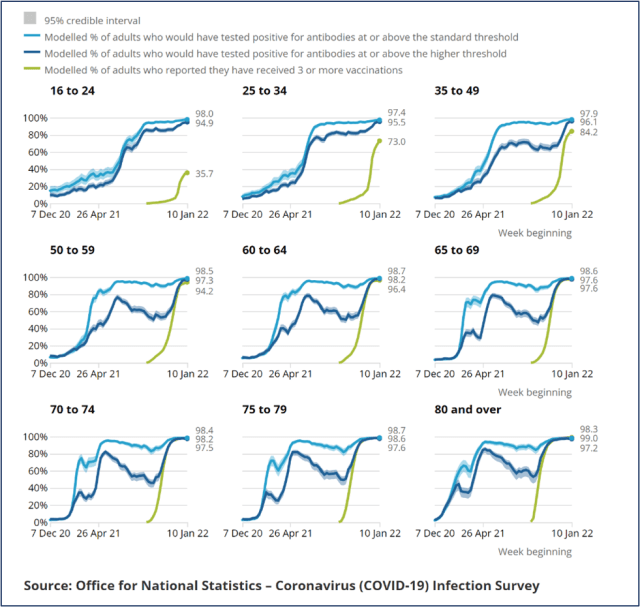
ONS Antibody Study (link)
The latest antibody study shows a sustained very high level of antibodies, both at the standard level (42ng/ml), and at the higher rate (179ng/ml) which it has been measuring recently. Across the UK as a whole, the proportion with antibodies is estimated as 98%.
Of particular encouragement is that these levels are being maintained at the older ages, despite the period since the booster jab now extending beyond three months. In the charts below we can see clearly how the booster jab restored and even enhanced levels beyond those observed after the second dose, and how they are being sustained, in contrast to the decline seen shortly after the second dose.
Ethnic Disparities in Mortality Continue into Third Wave (link)
This paper sets out to understand whether the ethnic variations in COVID mortality have continued into the third wave, and to what extent vaccine hesitancy in ethnic minorities may have accentuated the differences.
We know that various other demographic factors (particularly socio-economic) are highly correlated with ethnicity, and so a key part of the analysis was to adjust for these, and to adjust also for vaccination status, to see if there is any residual variance.
The results show that ethnic variations are indeed explained by many of the other demographic factors, but significant variations remain until vaccination status is adjusted for. However, for the majority of ethnic groups, the differences are no longer statistically significant when vaccination status is taken into account. The exceptions to this are for those of Bangladeshi ethnicity, and to a lesser extent males of Pakistani ethnicity, for whom the hazard ratios remain elevated.


SIREN Study Shows Vaccination Extends Protection of those with Natural Immunity (link)
A study of over 35,000 UK healthcare workers compares the protection (against PCR-confirmed infection) given by vaccination for those who have previously been infected and thus have natural immunity.
 The results show that whilst natural immunity on its own offered a high degree of protection for up to a year, beyond that there was considerable waning. In contrast, natural immunity plus vaccination appears to offer sustained immunity beyond the 12 month point.
The results show that whilst natural immunity on its own offered a high degree of protection for up to a year, beyond that there was considerable waning. In contrast, natural immunity plus vaccination appears to offer sustained immunity beyond the 12 month point.
The study predates Omicron, which has been shown to be more successful at escaping both natural and vaccine acquired immunity. Nevertheless, the study is a useful pointer towards the benefits of being vaccinated for those who have previously been infected.
Other
New COVID-19 measures will be outlined in the UK government’s “Living Safely With COVID” paper which is due to be published on 21 February. This will set out new COVID regulations for England, and the expectation is that all remaining regulations will be lifted, including the requirement to self-isolate following a positive test. It has also been widely reported in recent days that the UK Treasury is aiming to end free COVID testing by March 2022, ending PCR testing for most people with COVID symptoms (exceptions being those in hospitals, high-risk settings and those who are clinically extremely vulnerable). Under this approach, symptomatic people would receive either free lateral flow tests or no tests at all.
The group providing behavioural science advice to SAGE (SPI-B) issued a note in February (link) on the social impacts of lifting restrictions, including on testing and self-isolation.
Amongst other things, they noted:
- Policymakers should consider unintended consequences of changes to current testing provision, in particular mitigating economic and social harm to the clinically vulnerable and those from deprived socioeconomic and minority groups. For example, they note that it may be more difficult for these groups to seek medical treatment.
- Protective behaviours are likely to reduce or cease if they are not promoted over the longer term. Alongside the rationale for lifting restrictions, policymakers should continue to set out the importance of adherence to specific protective measures, emphasising the contribution of voluntary adherence to collective wellbeing and the ongoing risks to particular groups.
- Removal of free access to testing will make it harder for people to confirm infection and take actions to reduce transmission. This may increase anxiety in some people and limit their social participation, particularly if they are, or live with, someone who is clinically vulnerable.
- It is currently a legal requirement to self-isolate on a positive test – it is expected that this will become a matter of public health guidance. This will lead to ambiguity about the need for strict adherence. This is likely to affect vulnerable groups who will face greater pressure to work outside the home when ill.
They stress the importance of consistent messaging, and suggest moving the responsibility for this from central government to public health agencies to build on the strong public trust in the NHS in particular.
And Finally …
The C19-ARG team aren’t specialists in marine insurance, but news (link) caught our eye that the Felicity Ace, carrying nearly 4,000 cars, has caught fire. With no less than 189 Bentleys, Lamborghinis, and over 1,000 Porsches, we suspect that the insurance claim may be in excess of £100m if there is a full loss of the cargo.
We do hope that none of our readers have had disappointing news regarding the delivery of their new car this weekend, and on a more serious note, hope that Storm Eunice has not resulted in any other damage that might require a call to your helpful insurers.
Editor’s response;
From the High Seas to the Mill pond at Hurley, it’s been a bad week for boats!
Regulars on Lady Lucy will be saddened to hear that the helpful insurers will also be called into action following a tree falling on the boat as a result of Storm Eunice.

19 February 2022