Friday Report: Issue 40
By Dan Ryan and John Roberts COVID-ARG.com 
COVID-19 Actuaries Response Group – Learn. Share. Educate. Influence.


COVID-19 is still one of the hottest topics for scientific papers and articles. The COVID‑19 Actuaries Response Group provides a regular Friday update with a summary of key papers and articles.
Vaccines
Vaccinations for children
As vaccination programmes progress down priority groups and age bands, the focus has been on adults. This reflects both the risk and the exclusion of children from Phase 3 trials. However, there are now several ongoing trials focused on children. Pfizer/BioTech’s study recruited 3,000 children between ages 12 and 15 at the end of January, and Oxford Astrazeneca is monitoring 240 children between ages 6 and 17 (link).
On Tuesday, Moderna launched the largest clinical trial so far on children, KidCove, that will involve 6,750 children between the ages of 6 months and 11 years in the US and Canada. The trial will track the ability of the vaccine to prevent illness for 12 months after the second injection. A further trial is expected from Pfizer/BioNTech focused on children between ages 5 and 11. The intention of all of these trials is to provide sufficient evidence of efficacy to support possible vaccination programmes for the start of the next academic year.
Vaccine optimisation
Investigators have been using the OpenSafely-TPP platform to produce weekly reports on the roll-out of vaccines, identifying trends and differences by geography and also between key clinical and demographic patient groups. The latest study from 15 March highlights differences in the pace of vaccination in different groups, whilst recognising that the UK has one of the most successful vaccination programmes with very high levels of engagement. However, there is increasing international attention on whether vaccines are being targeted on those most in need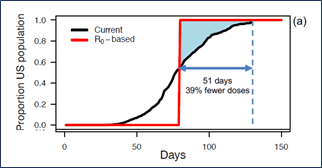
A US study considered whether different patterns of vaccine allocation could achieve universal herd immunity earlier. It estimates that distributing vaccines where the virus is spreading more quickly could achieve herd immunity within 2.5 months, and require 40% less vaccinations than the current strategy (with herd immunity estimated in 4.5 months).
Real-World Effectiveness Update (link)
PHE has published an update on the effectiveness it is seeing for both Pfizer and Astra-Zeneca vaccines in the real world (ie as opposed to clinical trials). It’s very clear that a single dose is offering protection of around 60% after 28 days, with very tentative signs that the A-Z effect continues to increase slowly beyond this.
In addition, for those who still get infected, there are further reductions in risk of those infections developing into hospitalisations, or ultimately death. The paper puts the overall effectiveness at 80% for hospitalisation and 85% for death. (The latter measure is only in relation to the Pfizer vaccine, with insufficient data yet for A-Z because of a 21st February data cut-off).
The reduction in infections is also a further encouraging sign that transmission will be reduced with fewer infections circulating in the community.
Vaccine Roll-out (link)
The latest weekly data shows how the roll-out continues to progress through the upper age groups in England.
All groups over 65 are now showing take-up in excess of 90%, and whilst there appears to be a slight downward trend as we move down the age-bands, there’s hope that the 60 to 64 group will also reach 90%.
Clinical and medical news
Cancer patients and efficacy of Pfizer/BioNTech vaccine
In our 7th Monthly Medical Update, we explored the time pattern of antibodies following single and double doses with the Pfizer/BioNTech vaccine, showing high rates 21 days after a single dose for all those under age 75 and for all ages if there had been a suspected prior COVID-19 infection.
A more recent pre-print study has looked at vaccine efficacy in cancer patients given concerns over vulnerability to COVID-19 because of immune suppression and exclusion of cancer patients with an active diagnosis from the previous Phase 3 vaccine clinical trials.
The study found that vaccine efficacy after a single dose was below 40% in patients with a solid tumour and below 15% for those with leukaemia, lymphoma or myeloma. Efficacy in the former group was boosted to over 95% if a vaccine booster was provided within 3 weeks. The numbers in the latter group were too small to support a similar conclusion. However, the study recommended the use of “ring vaccination” whereby those in close contact with the patient are prophylactically vaccinated, regardless of their own priority group status.
US Clinical Trial on the use of Convalescent Serum Therapy to treat COVID-19
In previous reports we have commented on the rationale and emerging evidence for the potential benefits of donated antibodies to prevent or limit the severity of symptoms in COVID-19 patients. The UK RECOVERY trial that considers a range of possible treatments shut recruitment to the convalescent plasma arm on 15 January (link) based on lack of evidence of change to 28-day mortality.
Convalescent serum therapy continues to be used in the USA under Emergency Use Authorisation. Earlier this week a double-blind RCT involving 223 patients and 5 hospitals in New York and Rio de Janeiro found no significant improvement in clinical status at 28 days but that 28-day mortality was significantly lower in those randomised to convalescent plasma (odds ratio 0.44, 95% CI 0.22-0.91). This result indicates that convalescent serum therapy will continue to be considered and evaluated.
Impact of lockdown on sleep and resting heart rates
Lockdowns across the world have disrupted almost every aspect of our lives, including our daily routines. A study of 113,000 users across 20 countries of the Oura ring sleep tracker over the period Jan-Jul 2020 investigated changes to sleep patterns and resting heart rate, and compared these with changes in lockdown stringency as measured by the Oxford Government Response Tracker.
Lockdowns might be expected to free up time and allow individuals to adopt preferred sleep/wake timings. However, at the same time we might expect lockdowns to increase anxiety and depression for many and hence reduce the quantity and quality of sleep. The study specifically looked at ‘midsleep’, or the middle hour of your sleep. The study found that more severe lockdowns delayed the time of midsleep, but also reduced midsleep variability and resting heart rates.
The following colourful figure illustrates the impacts across countries but also highlights the greatest pooled effects in April 2020 (gold symbol below) when stringency was highest in many countries.
Forest plots of average change in midsleep time, midsleep variability and resting heart rate
Data
ONS February Mortality Analysis (link)
The latest monthly analysis of mortality confirms the reduction from January’s second wave peak, although February still saw the third highest COVID mortality of the pandemic in England.
Although not represented by a graph in the report, the underlying data also shows the increase in age-standardised mortality over the last 12 months, which on a rolling 12 month basis is now back to a level last seen in February 2007.
ONS Antibody Survey (link)
 The latest fortnightly survey, for the four weeks to 3rd March, show antibody levels continuing to rise rapidly, most notably at the oldest age groups, as might be expected.
The latest fortnightly survey, for the four weeks to 3rd March, show antibody levels continuing to rise rapidly, most notably at the oldest age groups, as might be expected.
As an example, for age 75 to 79 in England has risen from 25% to 69%, and the 80+ group is now at 76%.
Given the time taken for antibodies to form, the earlier part of the analysis period is likely not to have the full effect yet for these age groups, so we can expect a further increase in the next report.
ONS Infection Survey (link)
As antibodies go up, in the other regular survey, infection levels are coming down, although the situation appears a little more variable than a week ago, with further falls in England and Wales, Northern Ireland holding steady, and an increase in Scotland, albeit within the bounds of the confidence intervals, so not yet clear.
In order:
- Scotland is now highest at 0.37% (+19%)
- Northern Ireland remains at 0.32%
- England has the largest fall to 0.29% (-22%)
- Wales is the lowest at 0.23% (-15%).
The age analysis shows falls in most age-groups, albeit of varying degrees, except for the youngest group.
The data relates to last week, so it would be too early to see any effect from the return of schools – next week’s report should provide some insight on that point.
European Comparisons (link)
In a busy week for the ONS, it’s also updated its comparison of excess mortality across Europe for the whole of 2020. The main feature is the second wave across Central and Eastern Europe in the Autumn, which has meant some countries, notably Poland, overtaking the UK in terms of overall impact.
The comparison of over and under 65s shows considerable variation, both in the trend in excess of time of the younger group, and in the alignment of the two groups. The UK is unusual in that both excesses move broadly in line across the year.
The analysis is (not unreasonably) only to end 2020. There has been some criticism that it doesn’t include early 2021 when the UK in particular suffered further very heavy mortality.

That is true, but whilst we now appear to be coming out of a period of excess mortality in the UK, the same is not the case for much of Western Europe, with further lockdowns now being imposed. Until we achieve much greater vaccine roll-out across Europe, any assessment of this nature will be premature.
“R” Estimate (link)
This week’s estimate by SAGE shows a slight increase from (0.6 to 0.8) to (0.6 to 0.9) for the UK, and a more probable increase from (0.6 to 0.8) to (0.7 to 0.9) for England. Significantly though, all areas remain with the upper bound at 0.9, suggesting that all areas are still falling.
And finally …
The group of universally understood words must have increased by at least one over the last year, with the word ‘Covid’ crossing all the frontiers that the underlying virus has, the word itself proving largely immune to translation. The word ‘actuary’ remains at the other end of the usage scale, perhaps regrettably to us, and we have not had to worry much about translation (at least in much of Europe, given the Latin origin noted even by Gibbon – attuarius, actuaire, attuario …) .
However, we were flattered to have our work mentioned at the Prime Minister’s press conference on Thursday with regard to vaccine priorities and deaths avoided. The IFoA was translated into American (Prof Whitty referred to the Society of Actuaries); the word ‘actuaries’ was translated in sign language as
“… ?”
It’s still unclear to us what the ‘signage’ for actuaries was – perhaps it was this combination of the number five and a look of bafflement? (circa 10 minutes into the clip)

?